In questo articolo dimostro che un test LTT per malattia di Lyme che utilizzi come uno degli antigeni la OspC (proteina integra) di B. burgdorferi sensu stricto può teoricamente risultare positivo (falso positivo) in soggetti con aumentata permeabilità intestinale.
Abstract
Some lymphocyte transformation tests (LTT) popular in Europe for the diagnosis of Lyme disease, use full-length OspC of B. burgdorferi as one of their antigens and request a positive stimulation index against only one or two antigens, in order to be considered positive. In what follows, we demonstrate that, in the case of patients with gut bacteria translocation, such a test has a theoretical risk of false positive results.
Lymphocyte transformation test
Lymphocyte transformation test (LTT) is an assay which allows measuring the activity of peripheral blood Th cells against specific antigens. T cell activation starts shortly after infection, with T cells proliferation and the production of cytokines (such as INF-γ) which regulate the adaptive immune response (Sompayrac, 2012). As T cell response vanishes after the resolution of the infection (Kaech, et al., 2007)↑, LTT may be useful in providing a proof of active infection. When an LTT assay is performed, Th cells from peripheral blood of a patient are exposed to proteins from a particular pathogen. If a significant reaction is noted, which could be either Th cells proliferation or INF-γ expression, the assay is considered positive and suggestive of an active infection by that particular pathogen. The response is expressed through a number, often referred to as stimulatory index (SI). In Lyme disease, several attempts have been made in order to obtain such a tool, either by T cells proliferation assays or by INF-γ measures (Dressler, et al., 1991)↑, (Chen, et al., 1999)↑, (Valentine-Thon, et al., 2007)↑, (von Baehr, et al., 2012)↑, (Callister, et al., 2016 May)↑. Nevertheless, this procedure has not been fully recognized as useful at present and neither the European guidelines (Stanek, et al., 2011)↑ nor the CDC (Centers for disease control and prevention, 2015)↑ recommend the use of this kind of test.

Th cells activation and cross-reactive T cell epitopes
Th cells are activated when their T cell receptors (TCR) recognize a complementary antigen presented by MHC II molecules (see Figure 1) (Sompayrac, 2012). Peptides presented by MHC II to T helper cells are exclusively linear epitopes, and they have a length between 13 and 17 amino acids (Rudensky, et al., 1991)↑. Various experiments have demonstrated that peptides with 5 identical amino acids in a sequence of 10 have good chances to represent cross-reactive T cell epitopes (Root-Bernstein, 2014)↑. That said, the algorithm described above for the LTT test is not free from the risk of false positive results, as each protein used as antigen could present one or more linear epitopes of 10 amino acids which share at least 5 amino acids with some epitope of 10 amino acids from another pathogen. This risk is particularly high when the assay uses complete proteins as antigens, and when a high SI for only a few antigens is required in order to have a positive result of the test.
OspC and Pseudomonas aeruginosa
We have used BLAST from NCBI (National Library of Medicine), with OspC from Borrelia burgdorferi (strain ATCC 35210 / B31 / CIP 102532 / DSM 4680) identified by the swiss-prot ID Q07337 (↑) as query sequence, settings being as follows: expected threshold of 10, BLOSUM62 as substitution matrix, and a word of 3 amino acids. We have built a custom database with the main Phyla of the human gut microbiome observed in a healthy population, which are Bacteroides, Firmicutes, Proteobacteria, Verrucomicrobia, Actinobacteria, Tenericutes, and Euryarchaeota (Giloteaux, et al., 2016)↑. One of the possible matches that BLAST gives back is the following alignment between the query sequence and the outer membrane protein G (OprG) of Pseudomonas aeruginosa (PDB ID: 2X27):

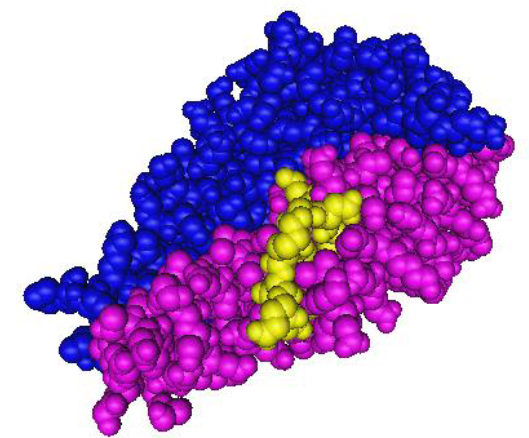
As you can see, we have 6 identical amino acids in a peptide 10 amino acids long. This means that this peptide from Borrelia burgdorferi could theoretically bind a Th cell previously activated by P. aeruginosa. Peptide 111-120 from OspC is reported in Figure 2. Peptide 51-60 of OrpG is in Figure 3. The 3D structure of OspC from B. burgdorferi strain B31 used for that picture has been experimentally determined with X rays and a resolution of 2,51 Å in 2001 (Kumaran, et al., 2001)↑ and its MMDB ID is 15958 (↑). The conclusion from this data is that Th cells from a patient with an active infection by P. aeruginosa could proliferate and produce INF-γ when exposed to OspC from B. burgdorferi. In other words, a patient with an active P. aeruginosa infection would come out to have a positive LTT test for OspC.

Gut bacteria translocation
A disrupted mucosal barrier of the bowel, with consequent translocation of bacteria from the gut to the peripheral blood, has been described in patients with liver diseases (Zhu, et al., 2013)↑, chronic HIV infection (Openshaw, 2009)↑, Crohn’s disease (Wyatt, et al., 1993)↑, and in myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) (Giloteaux, et al., 2016)↑. In ME/CFS it has been possible, in particular, to demonstrate the translocation of Pseudomonas aeruginosa, among other gram-negative enterobacteria. In fact serum concentration of IgA against lipopolysaccharides from P. aeruginosa and other enterobacteria has been found to be significantly greater in ME/CFS patients than in normal volunteers (Maes, et al., 2007)↑. Thus in ME/CFS patients the adaptive immune system usually reacts against pathogens which exit from the gut, and in particular, we know that it reacts against P. aeruginosa.
Conclusion
ME/CFS patients are among the main users of this kind of tests, because of the similarities between Lyme disease and the clinical picture of ME/CFS (Gaudino, et al., 1997)↑. ME/CFS patients have a high prevalence of increased gut permeability and gut microbiome translocation (Giloteaux, et al., 2016)↑, and their immune system reacts against P. aeruginosa in many cases (Maes, et al., 2007)↑. Thus, each LTT for Lyme disease which uses full-length OspC from B. burgdorferi ss as the antigen could theoretically lead to a high rate of false positive results in this population of patients. The Lyme disease LTT discussed above, which is currently popular in Europe, is one of such tests. More researches are warranted in order to confirm or exclude the theoretical danger of cross-reaction of Lyme disease LTT with gut microbiome. Moreover, on the basis of what here presented, it might be possible to develop an LTT specific for the diagnosis of gut bacteria translocation.
Donate
Consider supporting this website with a donation.
€1.00

Hi, My Italian is pretty bad – I would like to know how accurate this article could be and how did you come up with this theory
LikeLike
Hi LDN, thanks for reading. I have suggested in this paper that some LTTs for the detection of B. burgdorferi active infection might be falsely positive in subjects with gut flora translocation. This is only a theory, and should be validated or dismissed with proper experimental studies. How I have proposed this theory is explained in the article itself. As you know, LTTs for B. burgdorferi are not validated at present. There are some studies, but we don’t know how accurate those tests offered by various laboratories in Europe are.
LikeLike
interestting enough – I have done a western Blot (for Borrelia) that shows reactive bands P39 P 41 and P 100 but under the cut off criteria – so stated as negative – Then I have done a Melisa LTT test for metals and Borrelia – which comes back as “current Borrelia onfection” – BUT this test is (from my understanding) only done based on P 41 kDa band, which is not specific to borrelia (as you might know) – In a spermoculture, they found 500 UCI of E.Coli, and I have had gastric issues for 2 years that lead to Appendicectomy in Oct 2016. SO your theory could be right –
I am really trying to figure things out
LikeLike
The bands you reported above (P39, P41 and P100) are from the IgG westernblot or from the IgM one? Bands p39 and p100 are considered rather specific – in Europe – for the IgG response against B. burgdorferi. What Melisa LTT did you make? There is a new test LTT which has been recently developed in US, for Lyme disease, but I think it is not available, yet. It uses only specific peptides from B. burgdorferi antigens, instead of full length proteins. The test is the one described in this study: https://www.ncbi.nlm.nih.gov/pubmed/26936671
LikeLike
IGG Bands are P39 (0,2) – P41 (0,4) – P100 (0,6) and IGM are P41 (0,4) and P39 (0,3)
The Melisa Test I did is from a lab in germany Praxis Jochen Huter – but the numbers are quite low. To complicate things a bit more I am homozigous HLA DRB1 04 which seems to be the most “antibiotic resistant – chronic inflammation creative”
LikeLike
HLA-DRB1*0401 is relevant if you have arthritis, because it has been seen that patients with this genetic profile are more likely to develop an autoimmune arthritis, follwing Lyme disease infection, called ‘treatment resistant Lyme arhritis’. But if you do not have articular involvment, that genetic predisposition is not a problem. As for your westernblot, if the response was above the cut-off you would have a full positive westernblot, according to European guidelines. Nevertheless, seronegative Lyme does exist, and you should perhaps consider this possibility with your physician, if you have symptoms which might be related to Lyme disease.
LikeLike
I do have arhtritis, which is also quite dificult to diagnose – hum hum
As for the western blot, the KDa seems to be below the cut off involving 0 points so Negative diagnosis.
So right now I am still trying to figure what could be the cause of my health situation – and accepting the fact that maybe it’s not just one thing but several.
I have seen MANY physicians, and have had MANY opinions – but nothing crisp and clear. The hard part is not to follow the “they all suck” easy path, and remain positive about life
Thank you for taking the time to answer
LikeLiked by 1 person